The intricate relationship between postural alignment and physical health extends far beyond simple aesthetics or temporary discomfort. Modern understanding of biomechanics reveals that how you position your body throughout the day creates a cascade of physiological responses that can either support optimal function or gradually undermine your health over decades. Poor postural habits don’t merely cause occasional back pain; they fundamentally alter the mechanical stresses placed on your musculoskeletal system, potentially leading to degenerative changes, chronic pain conditions, and significant limitations in mobility as you age.
Research consistently demonstrates that postural deviations create compensatory patterns throughout the kinetic chain, affecting everything from breathing efficiency to digestive function. The human spine, designed to maintain specific curves that distribute load effectively, becomes compromised when subjected to prolonged abnormal positioning. This biomechanical dysfunction doesn’t remain localised but spreads throughout interconnected systems, influencing neural pathways, fascial networks, and even cardiovascular health in ways that many people never consider.
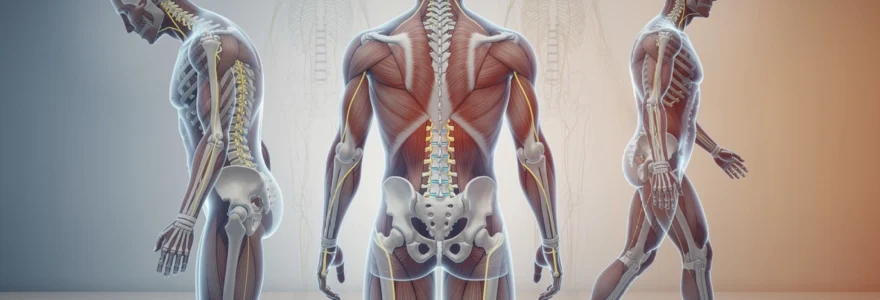
Biomechanical foundations of postural alignment and spinal kinematics
The spine functions as an integrated kinetic chain where movement and positioning at one segment directly influences adjacent and distant structures. Understanding this interconnectedness is crucial for appreciating how seemingly minor postural deviations can create significant long-term health consequences. The vertebral column’s natural curves—cervical lordosis, thoracic kyphosis, and lumbar lordosis—work synergistically to distribute mechanical loads efficiently whilst maintaining optimal shock absorption during movement.
Cervical lordosis and forward head posture impact on Atlanto-Occipital joint function
Forward head posture, increasingly common in our technology-driven society, fundamentally alters the biomechanics of the upper cervical spine. When the head translates forward from its optimal position over the shoulders, the atlanto-occipital joint experiences altered loading patterns that can compress neural structures and compromise blood flow to crucial brain regions. This positional change increases the mechanical load on posterior cervical muscles by up to 300% for every inch of forward head displacement.
The suboccipital muscles become chronically shortened and hyperactive, whilst deep neck flexors weaken through reciprocal inhibition. This muscular imbalance creates a self-perpetuating cycle where maintaining proper head position becomes increasingly difficult. Over time, these adaptations can lead to cervical disc degeneration, tension headaches, and even contribute to temporomandibular joint dysfunction through altered cervical-cranial mechanics.
Thoracic kyphosis alterations and vertebral compression forces
Excessive thoracic kyphosis, often accompanying forward head posture, places abnormal compression forces on the anterior aspects of thoracic vertebrae. This increased loading can accelerate disc degeneration and contribute to vertebral wedging, particularly problematic as bone density naturally decreases with age. The altered thoracic curvature also compromises respiratory mechanics by reducing chest expansion capacity and limiting diaphragmatic excursion.
When thoracic extension is restricted, compensatory movements occur at other spinal segments, particularly the cervical and lumbar regions. This compensation pattern can lead to hypermobility and eventual instability in areas not designed to handle excessive movement, creating a cascade of dysfunction throughout the entire spine.
Lumbar lordosis maintenance and sacroiliac joint stability
The lumbar lordosis serves as the foundation for proper spinal alignment, and its maintenance is critical for overall postural health. Loss of lumbar lordosis, common in prolonged sitting postures, increases intradiscal pressure by up to 40% compared to standing positions. This increased pressure accelerates disc degeneration and can lead to posterior disc bulging or herniation over time.
Lumbar spine positioning directly influences sacroiliac joint function through the close anatomical relationship between the lumbar spine and pelvis. When lumbar lordosis is compromised, the sacrum assumes an altered position within the pelvic ring, potentially creating asymmetrical loading patterns that can lead to sacroiliac joint dysfunction and associated pain syndromes.
Pelvic anterior tilt mechanics and hip flexor contracture
occurs when the pelvis rotates forward, increasing the curve in the lower back and shifting the body’s centre of gravity. Prolonged sitting, especially on non-ergonomic chairs, and repetitive hip flexion activities encourage the hip flexors to remain in a shortened position. Over time, this can lead to hip flexor contracture, where muscles such as the iliopsoas and rectus femoris lose their ability to fully lengthen. The result is a persistent pull on the front of the pelvis, exaggerating lumbar lordosis and increasing shear forces through the lumbar segments. This altered pelvic mechanics can also place additional stress on the knees and ankles, as the entire lower kinetic chain compensates for the shifted alignment.
For many people, an anterior pelvic tilt feels “normal” because the body has adapted to this posture over years. However, this chronic tilt reduces the efficiency of the gluteal muscles, disrupts sacroiliac joint stability, and can contribute to lower back pain and hamstring tightness. Addressing anterior pelvic tilt requires a combination of hip flexor stretching, glute and core strengthening, and conscious postural retraining during walking, standing, and sitting. As you begin to restore a more neutral pelvic position, load distribution through the lumbar spine and hips improves, supporting better long-term mobility and reducing the risk of degenerative changes in the lower back.
Musculoskeletal compensation patterns and adaptive shortening mechanisms
The body is remarkably adept at compensating for postural deviations, but these compensation patterns come at a cost. When one area of the body loses mobility or stability, another region often takes on extra work, leading to adaptive shortening in some muscles and overstretching in others. This process changes the resting length-tension relationships in muscles, alters joint mechanics, and can gradually shift normal movement patterns into dysfunctional ones. Over years, these musculoskeletal compensation patterns can contribute to chronic pain, reduced athletic performance, and diminished everyday function.
Understanding how these patterns develop helps you identify why certain areas feel perpetually tight while others seem weak or unresponsive. Rather than viewing pain as an isolated issue—for example, just a “tight neck” or “weak core”—we can see it as part of a larger postural strategy your body has adopted to keep you upright. Correcting posture-related imbalances therefore requires more than stretching what feels tight; it involves retraining movement patterns, improving joint alignment, and restoring balanced muscle function across the entire kinetic chain.
Upper crossed syndrome and levator scapulae hyperactivity
Upper crossed syndrome is a common postural distortion characterised by tight chest muscles (pectoralis major and minor) and overactive neck and shoulder elevators, coupled with weak deep neck flexors and scapular stabilisers. In this pattern, the head drifts forward, the shoulders round, and the upper back becomes excessively curved. The levator scapulae muscle, which elevates and downwardly rotates the scapula, often becomes chronically hyperactive to support the weight of the head and compensate for weak lower trapezius and serratus anterior muscles. This hyperactivity contributes to neck stiffness, shoulder discomfort, and tension-type headaches.
You can think of upper crossed syndrome like a tent with two overloaded guy lines at the front and back: as the lines tighten, the structure warps and strains. In the same way, tight levator scapulae and upper trapezius muscles pull the shoulder blades upward, while tight pectorals draw them forward, creating a compressed, internally rotated shoulder position. Correcting this long-term posture requires targeted strengthening of the mid-back and deep neck flexors, along with regular stretching and myofascial release of the chest, levator scapulae, and upper trapezius. Simple habits, such as pulling the shoulder blades gently down and back and aligning the ears over the shoulders during screen use, can significantly reduce strain on this region.
Lower crossed syndrome and gluteus maximus inhibition
Lower crossed syndrome mirrors the logic of upper crossed syndrome but occurs around the pelvis and lower spine. In this pattern, tight hip flexors and lumbar extensors are paired with weak or inhibited gluteus maximus and deep abdominal muscles. The result is an exaggerated lumbar lordosis and anterior pelvic tilt, which we often see in people who sit for long periods and then jump into high-intensity activities without proper conditioning. Over time, the brain relies increasingly on the lower back muscles and hamstrings to produce movements that should primarily involve the glutes, such as hip extension during walking, running, and lifting.
Gluteus maximus inhibition is particularly problematic because this muscle is a major powerhouse for propulsion and hip stability. When it does not activate effectively, the lumbar spine absorbs more load, and the sacroiliac joints may become stressed due to reduced pelvic control. Have you ever noticed your lower back working harder than your hips when you stand up from a chair or climb stairs? That is often a sign of this lower crossed pattern. Corrective strategies focus on lengthening the hip flexors, improving core stability, and re-educating glute recruitment through exercises like bridges, hip thrusts, and controlled squats with an emphasis on hip hinge mechanics.
Deep neck flexor weakness and suboccipital muscle tension
The deep neck flexors, including the longus capitis and longus colli, act as stabilisers for the cervical spine, maintaining proper alignment of the head over the shoulders. When these muscles become weak or underutilised—often due to prolonged forward head posture—the body compensates by over-recruiting superficial muscles such as the sternocleidomastoid and suboccipital group. The suboccipital muscles, positioned at the base of the skull, become tense and overworked as they attempt to keep the eyes level with the horizon despite poor head positioning. This leads to a constant low-grade contraction, contributing to headaches, dizziness, and neck stiffness.
A useful analogy is to imagine a small stabilising rope versus a large towing rope: when the stabiliser fails, the towing rope must take over, but it is not designed for fine control. In the same way, when the deep neck flexors are weak, the larger, more superficial muscles take on tasks they are not optimally designed to perform, resulting in inefficient movement and strain. Rehabilitation protocols typically include gentle “chin tuck” exercises to activate the deep neck flexors, combined with stretching and manual release of the suboccipital muscles. Over time, this helps restore a healthier alignment of the cervical spine and reduces the chronic tension that often accompanies desk-based work and extended screen time.
Psoas major tightness and reciprocal inhibition of gluteal complex
The psoas major is a deep hip flexor that connects the lumbar spine to the femur, playing a key role in both posture and movement. When you sit for extended periods, the psoas remains in a shortened position, gradually developing adaptive tightness. This tightness increases compressive forces on the lumbar vertebrae and can pull the spine into increased lordosis. Additionally, through a neurological process called reciprocal inhibition, chronic psoas activation can dampen the activity of the gluteal complex, especially gluteus maximus and medius, which are essential for hip extension and pelvic stability.
As the glutes become less active, the body compensates with increased use of the hamstrings and lumbar extensors to perform everyday tasks like walking, standing up, or climbing stairs. This not only raises the risk of lower back pain but can also contribute to hip and knee problems due to altered joint loading. To break this cycle, it is crucial to incorporate regular psoas and hip flexor stretching, particularly after long periods of sitting, and pair these stretches with focused glute activation exercises. By restoring balance between the psoas and the gluteal complex, you support better pelvic alignment, reduce stress on the lumbar spine, and promote more efficient movement patterns throughout the lower body.
Postural deviations and degenerative joint disease progression
Chronic postural deviations play a significant role in the development and progression of degenerative joint disease, including osteoarthritis and disc degeneration. When joints are repeatedly loaded in suboptimal positions, the articular cartilage and intervertebral discs experience uneven pressure, much like a car tyre that wears down more quickly on one edge when alignment is off. Over years, this asymmetric loading accelerates wear, reduces shock absorption, and can lead to joint space narrowing, osteophyte (bone spur) formation, and stiffness. Epidemiological studies indicate that individuals with pronounced spinal curvature abnormalities or knee malalignment have a substantially higher risk of early-onset osteoarthritis.
Posture-related joint stress is not limited to the spine; it extends to the hips, knees, and even smaller joints of the feet. For example, excessive anterior pelvic tilt and knee hyperextension can increase compressive forces on the patellofemoral joint, contributing to anterior knee pain and cartilage breakdown. Similarly, prolonged forward head posture raises compressive loads on the cervical discs, accelerating cervical spondylosis in susceptible individuals. By addressing faulty alignment early—through ergonomic adjustments, targeted exercise, and, when necessary, professional guidance—you can significantly reduce cumulative joint stress and help preserve mobility well into older age.
From a practical standpoint, monitoring how your body feels during and after common activities can offer clues about degenerative stress. Do your knees ache after standing at a counter, or does your neck feel compressed after working at a laptop? These sensations often reflect excessive joint loading caused by subtle postural errors. Interventions such as adjusting work surface height, optimising chair support, or modifying footwear can redistribute forces more evenly. Combined with strength and flexibility training, these adjustments help slow the progression of degenerative joint disease and support healthier, pain-free movement over the long term.
Fascial system dysfunction and myofascial trigger point development
The fascial system is a continuous, three-dimensional network of connective tissue that surrounds and interweaves with muscles, bones, nerves, and organs. When posture is optimal, fascia glides smoothly, distributing mechanical loads across the body much like a well-maintained suspension system. However, repetitive strain, sustained static postures, and previous injuries can cause areas of the fascial network to stiffen, adhere, or thicken. This fascial dysfunction restricts movement, alters force transmission, and can set the stage for myofascial trigger point development—localised hyperirritable spots within muscle and fascia that refer pain to other areas.
Trigger points often emerge in predictable patterns associated with poor posture. For instance, people with rounded shoulders and forward head posture commonly develop trigger points in the upper trapezius, levator scapulae, and pectoral muscles. These points can cause pain that radiates into the head, neck, or down the arm, making it difficult to identify the original source. You might think of fascia as a cling film wrapping around muscle; if parts of that film crumple or stick together, the entire wrap pulls unevenly, affecting distant regions. As a result, a fascial restriction near the hip can contribute to discomfort in the lower back, or tight plantar fascia in the foot can influence hamstring tension.
Addressing fascial system dysfunction involves more than simple stretching. Techniques such as myofascial release, foam rolling, trigger point therapy, and targeted manual therapy aim to restore glide and elasticity to the fascial network. Incorporating slow, controlled movements that explore full ranges of motion—such as in yoga, tai chi, or dynamic mobility routines—can further promote healthy fascial adaptation. For long-term postural health, combining these approaches with ergonomic improvements and strength training creates a comprehensive strategy that reduces trigger point recurrence and enhances overall tissue resilience.
Neurological implications of chronic postural stress on proprioceptive function
Posture is not solely a musculoskeletal issue; it is also deeply rooted in the nervous system through proprioception, the body’s ability to sense its position and movement in space. Proprioceptive input comes from receptors in muscles, tendons, joints, and fascia, which constantly send information to the brain about alignment and motion. When you maintain a specific postural distortion for long periods—such as slouching at a desk or standing with weight shifted to one side—the nervous system gradually accepts this position as the new “normal.” Over time, your internal map of what upright, neutral alignment feels like becomes distorted, making it harder to recognise and correct poor posture without external feedback.
Chronic postural stress can also contribute to altered sensory processing and muscle recruitment patterns. For example, sustained forward head posture and rounded shoulders change the way the brain coordinates neck, shoulder, and upper back muscles, often leading to co-contraction of multiple muscle groups that should work more independently. This not only reduces movement efficiency but may also heighten pain sensitivity, as nociceptive (pain) signals from overloaded tissues become more frequent. Research in neuroplasticity suggests that repeated movement patterns strengthen corresponding neural pathways, so habitual poor posture reinforces itself neurologically, much like practising a skill—but in this case, it is a “skill” that undermines long-term mobility.
Improving proprioceptive function is therefore a key component of any posture correction programme. Strategies include balance training, closed-eye alignment drills, and guided movement practices that emphasise body awareness, such as Pilates or mindful movement classes. Using mirrors, video recordings, or the guidance of a physiotherapist or movement specialist can provide visual and tactile feedback to help recalibrate your sense of neutral alignment. As your nervous system relearns what optimal posture feels like, maintaining healthier positions throughout the day becomes easier and more automatic, reducing the cumulative neurological and mechanical stress on your body.
Evidence-based corrective exercise protocols and manual therapy interventions
Given the complex interactions between posture, muscle balance, joint mechanics, and neurological control, effective intervention requires a structured, evidence-based approach. Modern corrective exercise protocols typically begin with a thorough assessment of alignment, mobility, and movement patterns, often using tools such as postural photography, functional movement screens, and range-of-motion testing. The goal is to identify not just where you feel pain, but which dysfunctional patterns across the kinetic chain contribute to that discomfort. Once these patterns are understood, practitioners can design targeted interventions that prioritise the most influential joints and muscle groups.
A comprehensive posture improvement plan usually combines mobility work, stability training, and motor control exercises. For example, someone with forward head posture and rounded shoulders might perform thoracic extension drills, deep neck flexor activation, and scapular stabilisation exercises, while also stretching the pectorals and upper trapezius. Similarly, an individual with anterior pelvic tilt and lower crossed syndrome would focus on hip flexor and lumbar mobility, combined with glute and core strengthening. Consistency is crucial: research indicates that performing corrective exercises several times per week for at least 8–12 weeks is often necessary to achieve lasting changes in alignment and movement habits.
Manual therapy can significantly enhance the effects of corrective exercise by addressing soft tissue restrictions and joint stiffness that limit optimal posture. Techniques such as joint mobilisation, spinal manipulation, soft tissue mobilisation, and myofascial release help restore normal motion and reduce pain, making it easier for you to adopt and maintain improved positions. For many people, a combined approach—working with a physiotherapist, chiropractor, or osteopath while following a home exercise programme—yields the best results. Think of manual therapy as “opening the door” by freeing up restricted tissues, and corrective exercise as “walking through the door” by retraining how you move and hold yourself in daily life.
From a practical standpoint, you can start applying evidence-based posture strategies by integrating short movement breaks, simple mobility drills, and low-load strengthening exercises into your routine. For example, performing chin tucks, scapular retractions, and hip flexor stretches for a few minutes every couple of hours can counteract the effects of prolonged sitting. Complement this with regular aerobic activity and whole-body strength training to support joint health and muscular endurance. As you become more aware of how posture influences your overall physical health and long-term mobility, these small, consistent actions accumulate, helping you maintain an active, resilient body well into later life.
 Good health cannot be bought, but rather is an asset that you must create and then maintain on a daily basis.
Good health cannot be bought, but rather is an asset that you must create and then maintain on a daily basis.
